UKALM Harley Street operates through a structured, escalation-based diagnostic model:
Pre-consultation intake → Targeted laboratory testing → Physician interpretation → Risk-stratified reporting → Defined review cycle
A cornerstone of the clinic’s model is the extended 120-minute longevity consultation, allowing comprehensive review of medical history, biomarker trends, lifestyle variables, and performance demands within a single structured session.
Diagnostic assessment may include:
- 55+ biomarker panels
- Cardiovascular and metabolic risk profiling
- Endocrine evaluation
- Glycaemic stability assessment
- Biological age modelling
- Microbiome or genomic insight where appropriate
The clinic functions within an extensive diagnostic ecosystem capable of supporting a broad range of laboratory investigations when clinically relevant. Test selection is guided by medical necessity rather than volume.
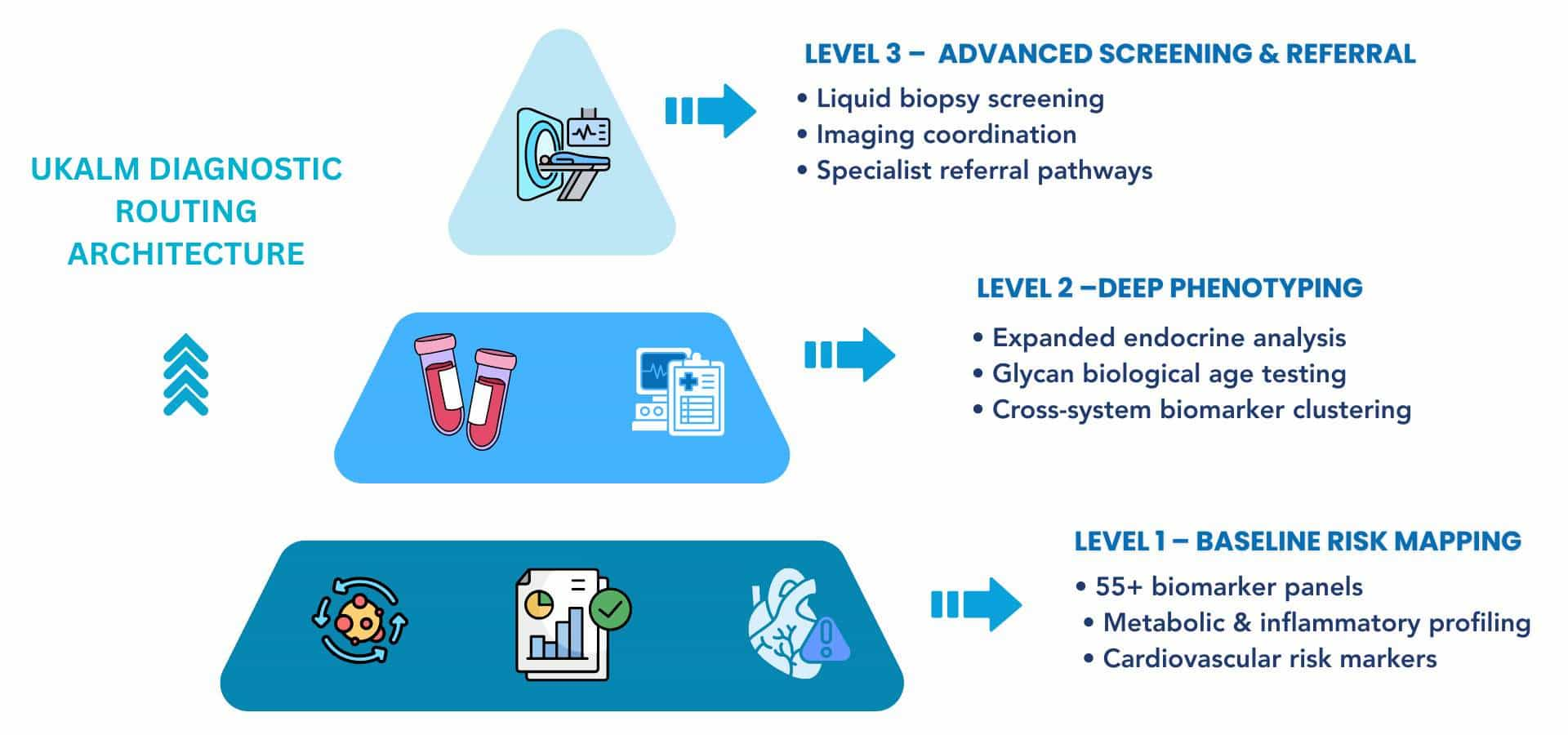
UKALM applies a three-level routing architecture:
- Level 1 – Baseline Risk Mapping:
Comprehensive multi-system biomarker profiling.
- Level 2 – Deep Phenotyping:
Expanded endocrine, metabolic, and biological age analysis with cross-system integration.
- Level 3 – Advanced Screening & Referral:
Molecular screening tools, imaging coordination, and structured specialist referral if pathology exceeds the preventive scope.
Escalation is clinically driven. Diagnostic intensity increases only when biomarker clustering or physician judgement supports deeper investigation.
Executive Time Efficiency
UKALM operates by appointment only. Diagnostic sequencing is organised to minimise fragmentation of time while preserving analytical depth. Multi-test coordination reduces repeated visits where possible, and structured reporting sessions are scheduled to align with professional commitments. Many individuals combine this with an executive health check for longevity for deeper insight.
Follow-up consultations may be conducted via secure telemedicine platforms when clinically appropriate. This enables continuity of oversight for individuals managing international schedules.
At a Glance – UKALM
|
Category
|
Details
|
|
Location
|
London, United Kingdom
|
|
Clinic Type
|
Private physician-led outpatient longevity clinic
|
|
Core Focus
|
Preventive medicine, biomarker profiling, biological age assessment, early risk screening
|
|
Typical Stay
|
Outpatient visits; no residential accommodation
|
|
Diagnostic Depth
|
55+ biomarker panels, biological age testing, liquid biopsy screening, advanced imaging coordination
|
|
Signature Method
|
Structured preventive routing model (Level 1–3 escalation)
|
|
Environment
|
Urban clinical setting
|
|
Privacy Level
|
UK regulatory compliance with structured data governance
|
|
Professional Recognition
|
Operates under regulated UK healthcare standards
|
Many visitors integrate consultations and diagnostic sessions into existing professional schedules rather than planning extended health stays. The clinic’s London location supports short, structured appointments within defined time blocks.
Accommodation is independent of clinic operations. Visitors typically arrange nearby business hotels or serviced apartments depending on travel logistics.
🔗 Explore nearby hotels & apartments
Executives and high-performing professionals typically seek structured medical clarity rather than lifestyle-oriented wellness environments. UKALM differentiates itself through defined diagnostic architecture, physician-led interpretation, and escalation-based screening models under UK medical regulation.
Key structural differentiators include:
- 55+ biomarker blood panels for metabolic, inflammatory, cardiovascular, renal, and endocrine assessment
- DNA-based biological age testing using glycan analysis
- Liquid biopsy screening technologies are designed to detect circulating tumour DNA signals
- Whole-body imaging coordination, where clinically appropriate
- Structured three-level routing architecture aligning diagnostic depth with risk indication
- Documented physician review cycles rather than automated reporting
The clinic separates diagnostics from outcomes. Laboratory findings are interpreted within a probabilistic framework. Biomarker deviation indicates system strain or risk tendency, not certainty of disease development or prevention. Many programs also focus on how to improve immune resilience for longevity.
Structural advantages include:
- Regulated UK medical governance
- Defined referral pathways when pathology exceeds the preventive scope
- Appointment-based outpatient model suitable for time-constrained professionals
- Clear escalation thresholds between baseline profiling and advanced screening
- Defined reporting intervals supporting longitudinal oversight
The clinic does not operate as a technician-led screening centre or protocol-driven optimisation facility. All diagnostic interpretation occurs under physician supervision, and escalation thresholds are clinically defined rather than commercially structured.
UKALM is structured around preventive medical governance rather than reactive treatment. The clinic’s stated purpose is to identify early biological deviation before the development of clinically diagnosable disease. This includes metabolic instability, inflammatory burden, cardiovascular risk markers, endocrine disruption, and cellular ageing indicators.
The clinic does not frame aging as a condition to be reversed. Instead, it approaches aging as a measurable biological trajectory influenced by cumulative stress exposure, metabolic regulation, genetic predisposition, and environmental variables. Biological age modelling and biomarker interpretation operate within probabilistic frameworks informed by observational research.
The objective is structured long-term planning support. Through repeat measurement, physician-led interpretation, and defined reporting cycles, individuals receive insight into trend movement rather than isolated laboratory interpretation. Risk assessment is directional, not deterministic.
The clinic does not frame preventive screening as urgent intervention. Its model is structured around continuity and longitudinal review rather than rapid corrective intensity. Oversight is designed to support measured, informed executive decision-making over time.
Clinical Purpose
The clinic’s clinical purpose can be summarised across three structured pillars:
Early Risk Identification
Identification of metabolic, inflammatory, endocrine, cardiovascular, and cellular strain patterns before diagnostic disease thresholds are crossed.
System-Level Understanding
Integration of cardiovascular, glycaemic, hormonal, inflammatory, renal, and age-related biomarkers within a unified interpretive framework rather than siloed specialty review.
Long-Term Planning Support
Defined physician review cycles that monitor biomarker trajectory over time, enabling recalibration when clinically indicated.
This framework supports measurement-based oversight. It does not guarantee disease prevention, reversal, or outcome certainty.
Who This Clinic Is Designed For
UKALM is structured for individuals seeking analytical oversight rather than symptom-driven episodic care.
The clinic is designed for:
- Executives managing sustained cognitive and operational load
- Founders and entrepreneurs under chronic stress exposure
- Investors requiring structured long-term health risk mapping
- Professional athletes seeking metabolic and recovery profiling
- High-performers seeking clarity on biomarker trajectory rather than treatment of acute illness
It is not positioned for emergency medicine, inpatient care, or acute disease management. Individuals with established pathology requiring specialist intervention are referred appropriately.
Focus Areas
|
Focus Area
|
What This Means in Practice
|
|
Medical Discipline
|
Preventive longevity medicine under regulated UK physician oversight
|
|
Core Biological System
|
Metabolic, inflammatory, cardiovascular, endocrine, and cellular ageing systems
|
|
Environment & Design
|
Outpatient urban clinical setting; appointment-based structure
|
|
Program Structure
|
Three-level routing architecture with defined escalation thresholds
|
|
Lifestyle as Medicine
|
Structured discussion of nutrition, sleep, metabolic regulation, and stress exposure within physician review cycles
|
|
Privacy
|
UK regulatory compliance with controlled-access data governance
|
|
Long-Term Strategy
|
Repeat measurement, physician interpretation, and longitudinal risk mapping
|
UKALM frames its clinical approach within a preventive model often described as “Medicine 2.0.” This distinguishes structured risk identification from traditional reactive care models.
Reactive medicine typically intervenes after disease thresholds are met when laboratory values fall outside reference ranges or when symptoms become clinically significant. Preventive longevity medicine, by contrast, focuses on deviation patterns that precede diagnosable disease.
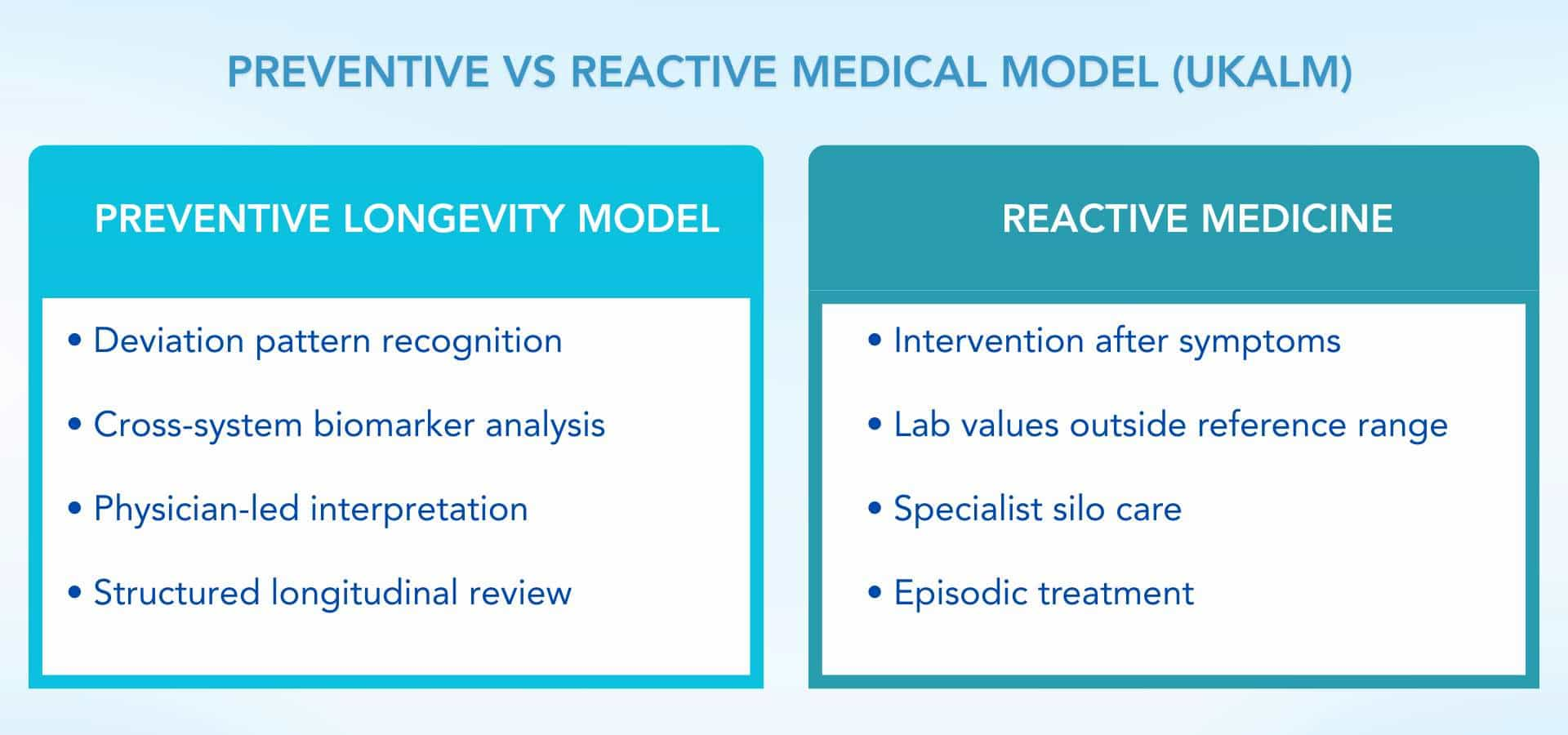
UKALM applies systems-based interpretation rather than isolated marker correction. Biomarkers are reviewed across metabolic, cardiovascular, inflammatory, endocrine, and cellular aging domains. Physician interpretation remains central. Raw laboratory outputs are not treated as conclusions.
The clinic deliberately avoids trend-driven interventions or unvalidated technologies. Escalation to advanced screening tools occurs only when clinical context supports additional depth. Measurement precedes intervention, and interpretation precedes decision-making.
Screening technologies and biological age modelling are incorporated within established clinical and regulatory boundaries. They are not positioned as performance tools, investigational therapies, or experimental interventions. Interpretation precedes decision-making, and escalation remains governed by physician oversight.
Core System Focus
UKALM places primary emphasis on metabolic and inflammatory regulation as coordinating systems influencing long-term health trajectory.
This includes structured evaluation of:
- Glycaemic stability (fasting glucose, HbA1c, insulin dynamics)
- Inflammatory markers (including CRP and related indicators)
- Lipid metabolism and cardiovascular risk markers
- Renal and hepatic function
- Endocrine regulation
- Biological age modelling through glycan-based DNA analysis
Rather than isolating a single abnormal marker, the clinic assesses interaction patterns across these systems.
|
🔍 Did You Know?
Longitudinal analyses (e.g., Moffitt et al., 2017) demonstrate that accelerated biological aging markers are associated with increased risk of transitioning from single chronic conditions to multimorbidity. These findings support early risk mapping but do not predict individual outcomes.
|
Lifestyle as a Medical Tool
Within UKALM’s framework, lifestyle variables are treated as measurable inputs influencing biomarker trajectories rather than motivational themes.
Physician discussions may address:
- Nutritional structure aligned with glycaemic regulation
- Sleep architecture and recovery cycles
- Muscle mass preservation and metabolic resilience
- Stress exposure patterns
- Cardiovascular conditioning
Lifestyle recalibration is discussed within reporting sessions and reviewed against subsequent biomarker changes during follow-up cycles.
|
🔍 Did You Know?
Observational research has associated sustained physical activity with more favourable aging biomarker profiles, though causality and magnitude of effect remain under investigation in longitudinal studies.
|
UKALM operates within a diagnostics-first framework aligned with the Medicine 3.0 longevity model. Clinical interpretation begins with structured measurement rather than symptom-driven assumption. The objective is to identify biological deviation patterns across metabolic, inflammatory, cardiovascular, endocrine, and cellular ageing systems before disease thresholds are crossed.
Diagnostic depth is determined by clinical indication and executive objectives. Not all individuals undergo maximum-level screening. Escalation follows relevance and risk stratification rather than fixed protocol intensity.
Measurement is separated from outcome claims. Biomarker findings indicate directional risk patterns, not certainty of disease development or prevention.
Diagnostic Assessment Includes
Depending on the clinical context, assessment may include:
- Extended biomarker panels (55+ parameters, including inflammatory, metabolic, lipid, renal, and endocrine markers)
- Cardiovascular risk profile, including advanced lipid markers
- High-sensitivity C-reactive protein (hs-CRP)
- Glycaemic markers (fasting glucose, HbA1c, insulin dynamics)
- DNA-based biological age testing using glycan analysis
- Liquid biopsy screening technologies assessing circulating tumour DNA signals
- Advanced imaging coordination where clinically indicated
All laboratory outputs undergo physician interpretation. Individual values are not treated as standalone conclusions. Pattern recognition across systems informs reporting.
|
🔍 Did You Know?
Emerging research into circulating tumour DNA suggests that liquid biopsy technologies may detect molecular signals associated with early-stage pathology. These tools remain adjunctive screening methods and do not replace diagnostic imaging or specialist evaluation.
|
Chronomedicine & Future Risk Mapping
UKALM incorporates temporal pattern recognition into its oversight model. Biomarker values are assessed across time rather than as isolated data points. This approach aligns with principles of chronomedicine, where trend movement may provide more insight than a single measurement.
Future risk mapping is probabilistic. Biological age acceleration, inflammatory burden, glycaemic instability, and lipid deviation are interpreted as directional indicators. They inform structured planning but do not predict certainty.
The reporting cycle follows a defined structure:
Baseline measurement → Physician interpretation → Defined review interval → Trend reassessment
This iterative model supports long-term oversight rather than episodic intervention.
UKALM’s strengths lie in structured interpretation, escalation-based diagnostics, and physician-governed review cycles rather than procedural intensity or intervention volume. The clinic positions itself around measurement architecture and longitudinal oversight.
Below are three defined areas of medical strength.
Key Medical Strength 1 – Integrated Multi-System Risk Profiling
UKALM integrates metabolic, cardiovascular, inflammatory, endocrine, renal, and cellular ageing markers within a single interpretive framework. Rather than correcting isolated laboratory deviations, physicians assess interaction patterns across systems.
For example:
- Glycaemic instability is interpreted alongside inflammatory load and lipid markers
- Biological age modelling is reviewed in the metabolic and cardiovascular context
- Endocrine markers are evaluated against stress exposure and sleep variables
This cross-system analysis reduces the risk of overcorrecting single abnormal values without understanding broader physiological interaction.
|
🔍 Did You Know?
Cohort research indicates that clustering of metabolic and inflammatory abnormalities increases long-term disease risk more significantly than isolated marker deviation. This supports system-level interpretation rather than single-value correction.
|
Key Medical Strength 2 – Biological Age & Early Screening Integration
UKALM incorporates DNA-based biological age testing and liquid biopsy screening technologies within a structured escalation model.
Biological age modelling provides directional insight into cellular aging trajectory. Liquid biopsy screening technologies aim to detect circulating molecular signals associated with early-stage pathology. These tools are used as adjunctive risk indicators rather than diagnostic conclusions.
The clinic separates screening from certainty. Abnormal findings trigger structured follow-up and, when appropriate, specialist referral.
This integration supports early risk identification within regulated medical oversight.
Key Medical Strength 3 – Structured Review & Escalation Framework
UKALM operates under a three-level routing model that aligns diagnostic depth with clinical indication:
Level 1 – Baseline Risk Mapping
Level 2 – Deep Phenotyping
Level 3 – Integrated Screening & Referral
Escalation occurs only when relevant clinical signals justify increased diagnostic intensity.
The review cycle follows a defined sequence:
Measurement → Interpretation → Reporting → Scheduled Reassessment
Escalation between levels is triggered by predefined biomarker deviation, cumulative inflammatory or metabolic clustering, emerging imaging findings, or physician clinical judgement. This decision architecture prioritises relevance over intensity and ensures screening depth aligns with clinical indication rather than fixed protocol sequencing.
The following summaries reflect patient experiences described within published clinic materials. They illustrate diagnostic sequencing and physician-led interpretation rather than guaranteed results. Outcomes vary based on baseline health status, genetics, adherence, and environmental exposure.
Outcome 1 – Persistent Fatigue with Normal Routine Testing
Before:
An executive reported ongoing fatigue, reduced cognitive clarity, and decreased exercise tolerance despite routine primary care testing remaining within standard reference ranges.
After:
Expanded biomarker profiling identified iron deficiency, suboptimal vitamin status, and metabolic strain indicators. Following structured physician-led review and monitored recalibration, the individual reported improved energy stability over subsequent review cycles.
Source:
Clinic-published patient experience summary.
Outcome 2 – Early Metabolic Risk Detection
Before:
A professional undergoing baseline screening presented without overt symptoms but demonstrated elevated inflammatory markers and early glycaemic instability on extended testing.
After:
Through structured monitoring, dietary recalibration discussion, and follow-up assessment, biomarker trends showed movement toward improved metabolic regulation across defined review intervals.
Source:
Clinic-published patient experience summary.
|
⚠️ Editorial Note
These outcomes reflect individual experiences reported within the clinic’s published materials. Results vary. Diagnostics indicate biological risk patterns, not certainty of disease development or prevention. Observed changes depend on individual baseline physiology, adherence to physician guidance, and external factors. Preventive longevity medicine supports structured oversight rather than guaranteed outcomes.
|
UKALM structures its programs around diagnostic sequencing and physician interpretation rather than fixed treatment packages. Programs are outpatient-based and customised following baseline assessment. They are not residential retreats and do not operate on a spa model.
Durations reflect typical engagement frameworks rather than guaranteed timelines. Diagnostic depth and review intervals are determined by clinical indication and executive objectives.
Comprehensive Longevity Assessment (2–4 Weeks)
Format:
Outpatient diagnostic sequencing followed by structured physician reporting.
Clinical Focus:
Baseline risk mapping across metabolic, inflammatory, cardiovascular, endocrine, and cellular ageing domains.
Diagnostics May Include:
- 55+ biomarker blood panels
- Cardiovascular risk profiling
- Glycaemic and inflammatory markers
- DNA-based biological age testing (glycan analysis)
- Structured health risk assessment
Program Structure:
Pre-visit intake → Laboratory testing → Physician interpretation session → Risk-stratified reporting → Defined follow-up interval
Follow-up reassessment typically occurs within defined review intervals, allowing structured comparison against baseline measurement and enabling trajectory-based interpretation rather than isolated evaluation.
Advanced Preventive Screening Pathway (4–8 Weeks)
Format:
Escalation-based diagnostic pathway integrating advanced screening technologies where clinically indicated.
Clinical Focus:
Deep phenotyping and early-stage risk detection across multi-system domains.
Diagnostics May Include:
- Extended biomarker profiling
- Liquid biopsy screening technologies
- Advanced imaging coordination
- Endocrine and metabolic expansion panels
- Longitudinal trend reassessment
Program Structure:
Baseline measurement → Escalation to Level 2 or Level 3 diagnostics (if indicated) → Physician reporting → Structured review cycle
Advanced screening tools are adjunctive and operate within probabilistic frameworks. Abnormal findings trigger further evaluation or referral rather than immediate intervention.
Follow-up reassessment typically occurs within defined review intervals, allowing structured comparison against baseline measurement and enabling trajectory-based interpretation rather than isolated evaluation.
UKALM operates as a private outpatient medical clinic in London. It does not provide inpatient admission, residential recovery stays, or retreat-style programming. All services are delivered through scheduled consultations, structured diagnostics, and defined review cycles under regulated UK healthcare standards.
Interventions are considered only after physician's interpretation of laboratory findings. The clinic does not position itself around high-volume procedures or trend-driven therapies. Measurement precedes discussion.
Medical & Restorative Therapies
Therapies discussed within UKALM’s framework may include:
- Structured nutritional recalibration under physician review
- Targeted supplementation based on laboratory findings
- Continuous Glucose Monitoring (CGM) for glycaemic variability assessment
- Hormone evaluation and, where clinically indicated, conventional therapies within established medical guidelines
- NAD-related metabolic support strategies within regulated scope
- Cardiovascular and metabolic risk reduction discussions aligned with biomarker findings
Conventional pharmacologic therapies are prescribed only within established UK medical standards and when clinically indicated. Preventive screening does not substitute specialist management of established disease. Therapeutic decisions remain subject to physician evaluation and regulatory governance.
Clinical Facilities
UKALM functions as an urban outpatient clinic. Laboratory diagnostics are conducted through accredited external laboratory partners operating under recognised quality assurance frameworks.
On-site consultations focus on:
- Physician-led reporting sessions
- Interpretation of extended biomarker panels
- Review of biological age modelling outputs
- Discussion of screening results
- Structured risk mapping conversations
Advanced imaging and specialist diagnostics are coordinated externally when indicated. The clinic does not operate inpatient wards or surgical theatres.
Architecture, Environment & Digital Discipline
The clinic operates within a professional urban medical setting in London. It is not a spa or lifestyle venue. The environment prioritises privacy, discretion, and structured consultation.
Digital governance follows UK regulatory standards. Laboratory data, biological age modelling outputs, and clinical notes are stored within secure, controlled-access systems compliant with applicable data protection regulations.
The outpatient structure enables patients to integrate visits into professional schedules without requiring extended absence from work or travel disruption. For a broader comparison, see the best longevity clinics in the UK.
UKALM structures pricing around diagnostic depth, physician interpretation time, and defined review cycles. The clinic does not operate on volume-based packages or promotional pricing models. Fees reflect the scope of laboratory testing, screening coordination, and physician reporting sessions.
Costs vary depending on the level of diagnostic assessment selected and the complexity of follow-up required. Supplementation, prescription medications, advanced imaging, or specialist referrals are billed separately where applicable.
No program guarantees specific health outcomes. Pricing reflects structured medical oversight within a probabilistic risk framework.
Pricing
|
Category
|
Details
|
|
Clinic Positioning
|
Private physician-led outpatient longevity clinic
|
|
Stay Length
|
Outpatient visits; no residential accommodation
|
|
Entry Pricing
|
Provided following consultation planning and diagnostic scoping
|
|
What’s Included
|
Selected laboratory testing, physician interpretation session, structured reporting
|
|
Additional Costs
|
Supplements, prescription therapies, advanced screening, imaging coordination, specialist referrals
|
|
Program Structure
|
Baseline measurement → Physician review → Defined follow-up cycle
|
|
Clinical Principle
|
Measurement-driven oversight within regulated UK medical governance
|
UKALM does not operate on subscription-based membership commitments. Engagement is structured around defined diagnostic cycles, allowing individuals to determine scope and review intervals according to clinical indication and personal objectives.
How Programs Are Structured
Programs follow a defined workflow:
Pre-visit preparation:
Medical history intake and structured diagnostic planning.
On-site diagnostics:
Laboratory sampling and coordinated screening where indicated.
Physician interpretation:
Comprehensive reporting session integrating cross-system biomarker analysis.
Reporting & follow-up:
Defined review interval assessing trend direction and recalibration where appropriate.
This structure separates measurement from decision-making and emphasises physician governance over automated output. These structured pathways are similar to executive longevity testing packages designed for high performers.
Length of Stay
UKALM operates exclusively as an outpatient clinic.
- No inpatient admission
- No residential accommodation
- No retreat-style programming
Initial diagnostic appointments are typically completed within scheduled consultation blocks. Follow-up reviews may be conducted remotely when clinically appropriate.
The clinic is designed to integrate within professional schedules rather than require extended absence from work.
UKALM is located in London, United Kingdom. The clinic operates strictly by appointment and does not provide residential accommodation. It functions as an outpatient medical facility designed to integrate with professional schedules rather than require extended stays.
Many visitors coordinate consultations alongside existing business travel or professional commitments. The appointment-based structure allows diagnostic sequencing and reporting sessions to be completed within defined time windows.
Recommended Length of Stay
As an outpatient clinic, UKALM does not require overnight stays.
Initial diagnostic appointments are typically completed across one or two scheduled visits, depending on the scope of laboratory testing and screening coordination. Physician reporting sessions may occur separately and can be conducted remotely where clinically appropriate.
Duration of engagement depends on the depth of assessment selected and the interval between structured review cycles.
How to Reach the Clinic?
UKALM is accessible via London’s major transport infrastructure.
Nearest Airport:
London Heathrow Airport
Typical Transfer Time:
Approximately 30–45 minutes by car, depending on traffic conditions
Transport Options:
Private car service, taxi, underground rail, or national rail connections
For travel planning convenience:
🔗 Find best flights to London
🔗 Find car rentals in London
Links provided for travel planning convenience only.
Accommodation & Stay Planning
UKALM does not operate on-site accommodation. Visitors travelling from outside London typically arrange independent lodging nearby.
Central and West London offer business-oriented hotels and serviced apartments suitable for short stays aligned with consultation schedules. Many guests select accommodation within a convenient distance of the clinic to minimise travel time between appointments. You can also explore the best longevity clinics in London to compare similar providers.
🔗 Explore nearby hotels & apartments
What to Bring
Visitors are advised to bring:
- Prior laboratory results (if available)
- Current medication list
- Relevant imaging reports
- Personal identification
No specialised equipment or athletic gear is required unless advised during pre-visit planning.
The preventive longevity sector remains heterogeneous. There is no globally standardised framework governing private longevity clinics. Models range from wellness-oriented centres to highly medicalised outpatient facilities. As a result, executive due diligence requires evaluation of physician leadership, regulatory governance, diagnostic specificity, and structured review architecture.
UKALM positions itself as a physician-led outpatient clinic operating within regulated UK healthcare standards. Its model centres on structured biomarker profiling, biological age testing, liquid biopsy screening technologies, and escalation-based diagnostic routing. Interpretation is physician-led, not technician-driven or automated.
Longevity medicine operates within probabilistic frameworks. Associations between biological age acceleration, inflammatory burden, metabolic instability, and multimorbidity are supported in longitudinal research. However, these associations do not predict individual certainty. Screening technologies provide directional insight rather than guaranteed outcomes.
Within the broader sector, UKALM’s positioning can be characterised by:
- Physician-led governance under UK regulation
- Three-level diagnostic routing architecture
- Escalation-based screening rather than fixed intervention intensity
- Defined review cycles supporting longitudinal oversight
- Structured referral pathways when pathology exceeds the preventive scope
Unlike direct-to-consumer biological age testing platforms or wellness-oriented longevity centres, UKALM integrates screening technologies within regulated physician governance and structured referral architecture. Screening is embedded within clinical oversight rather than delivered as standalone consumer testing.
What Patients Commonly Report
Themes described within published materials include:
- Increased clarity regarding metabolic and inflammatory risk markers
- Identification of previously unrecognised nutrient or hormonal deviation
- Greater understanding of cardiovascular and glycaemic risk trajectory
- Structured planning discussions informed by biological age modelling
These reports reflect individual experiences and do not indicate uniform outcomes.
Media & Professional Recognition
UKALM has been referenced in longevity and preventive health discussions within the UK private healthcare sector. Its positioning within the “Medicine 2.0” framework aligns with emerging discourse around preventive governance and biological age modelling.
Professional credibility is derived from regulated UK medical oversight and defined diagnostic infrastructure rather than lifestyle branding.
UKALM operates within a segment of the longevity sector that prioritises structured measurement over narrative positioning. In a field often characterised by lifestyle framing or trend-driven terminology, the clinic’s model centres on extended biomarker profiling, biological age assessment, escalation-based screening, and physician-led interpretation.
Longevity medicine remains evidence-evolving. Associations between inflammatory burden, metabolic instability, biological age acceleration, and long-term disease risk are supported by longitudinal research. However, prediction at the individual level remains probabilistic. No screening model eliminates biological variability or guarantees prevention.
Within that limitation, UKALM’s value proposition is governance rather than promise. Baseline mapping, structured reporting, and defined reassessment intervals provide data-informed insight without requiring residential stays or extended professional disruption.
For executives, founders, investors, and high-performing professionals, relevance lies in clarity of interpretation. The clinic does not position itself as a cure model or performance enhancement environment. It offers structured preventive oversight under regulated UK medical standards, separating diagnostics from outcomes and emphasising documented review over narrative assurance. This reflects trends seen across the best longevity clinics in Europe.
Is UKALM a medical clinic or a wellness centre?
UKALM operates as a physician-led outpatient medical clinic under regulated UK healthcare standards. It is not a spa, retreat, or lifestyle centre. Diagnostic sequencing, screening interpretation, and reporting are conducted under medical oversight.
Lifestyle variables such as nutrition, sleep, and metabolic regulation are discussed within a clinical framework. The clinic does not provide recreational wellness services.
Who is the clinic designed for?
The clinic is structured for executives, founders, investors, professional athletes, and high-performing individuals seeking structured insight into biomarker trends and long-term risk mapping.
It is not positioned for emergency care, inpatient treatment, or acute disease management.
How personalised is the process?
Personalisation begins with diagnostic depth. Testing may include extended biomarker panels, biological age assessment, liquid biopsy screening technologies, and advanced metabolic profiling when clinically indicated.
Interpretation is physician-led. No fixed protocol is universally applied. Personalisation refers to diagnostic sequencing and structured review cycles rather than experimental treatment variation.
How is patient privacy handled?
UKALM operates under UK medical regulatory standards and applicable data protection laws. Laboratory results, biological age modelling outputs, and clinical documentation are stored within secure, controlled-access systems.
Data is used exclusively for clinical interpretation and is not distributed without appropriate consent.
Can patients remain connected and working during programs?
Yes. The outpatient structure allows consultations to be integrated within professional schedules. Follow-up reporting sessions may be conducted remotely where clinically appropriate.
There is no inpatient admission or residential requirement.
Does the clinic treat diabetes or chronic conditions?
The clinic focuses on preventive risk mapping and biomarker interpretation. It does not replace specialist care for established chronic disease.
If diagnostic findings indicate pathology beyond the preventive scope, referral to appropriate medical specialists is advised. All medical decisions should be made in consultation with a qualified personal physician.
How should value be evaluated relative to cost?
Value is derived from diagnostic depth, physician interpretation time, and structured review cycles rather than isolated interventions.
The clinic’s model supports long-term oversight and risk transparency. It does not guarantee disease prevention or lifespan extension.
A Strategic Pause That Protects Long-Term Performance
In high-performance environments, uncertainty is rarely ignored. Financial exposure, operational volatility, and competitive risk are measured, reviewed, and managed through structured oversight. Biological systems operate under similar principles, though their signals are often less visible until deviation becomes clinically significant.
UKALM positions its work within a preventive framework built on extended biomarker profiling, biological age modelling, escalation-based screening, and physician interpretation. It does not promise reversal of aging or elimination of disease risk. It provides structured insight into metabolic, inflammatory, cardiovascular, endocrine, and cellular ageing patterns that may influence long-term trajectory.
Longevity medicine remains evidence-evolving. Associations between biological markers and future disease risk are supported in cohort research, yet individual prediction remains probabilistic. Screening technologies and biomarker analysis inform directional understanding rather than certainty.
For executives, founders, investors, and high-performing professionals, the relevance lies in governance. Baseline measurement, structured reporting, and defined reassessment intervals allow health risk to be reviewed with a similar discipline applied to other strategic domains.
Preventive oversight, when approached conservatively, is less about intensity and more about continuity.
👉 View Longevity Program
↩ Return to ExtendMy.Life
↑ Back to Top
Disclaimer
This page is provided for informational and editorial purposes only. It is intended to support structured review and informed executive decision-making regarding preventive longevity services. It does not constitute medical advice, diagnosis, or treatment.
Reading this content does not establish a doctor–patient relationship with UKALM, its physicians, or ExtendMy.Life. Clinical services are delivered only through formal consultation, medical history review, and individual physician assessment.
Longevity medicine and biological age modelling operate within probabilistic frameworks. Associations between biomarkers, inflammatory burden, metabolic regulation, and long-term disease risk are primarily derived from observational and longitudinal cohort research. These associations describe population-level trends and do not guarantee individual outcomes.
Diagnostic findings represent biological patterns and directional risk indicators, not certainty of disease development or prevention. Screening technologies, including biological age testing and liquid biopsy methodologies, are adjunctive tools and may require further evaluation if abnormal findings arise. Individual results vary based on genetics, lifestyle, environmental exposure, baseline physiology, and adherence to physician guidance.
UKALM operates within regulated UK medical governance. Where diagnostic findings suggest pathology beyond preventive scope, referral to appropriate specialists may be recommended. Preventive screening does not replace specialist care for established medical conditions.
All medical decisions, including laboratory testing, prescription therapies, supplementation, lifestyle modification, or advanced screening, should be made in consultation with a qualified personal physician. ExtendMy.Life does not provide medical services and does not recommend specific treatments.
This page separates editorial analysis from clinical care and should not replace personalised medical consultation.
References
Belsky, D.W. et al. (2015) ‘Quantification of biological aging in young adults’, Proceedings of the National Academy of Sciences, 112(30), pp. E4104–E4110.
Ferrucci, L. and Fabbri, E. (2018) ‘Inflammageing: chronic inflammation in ageing, cardiovascular disease, and frailty’, Nature Reviews Cardiology, 15(9), pp. 505–522.
Franceschi, C. et al. (2018) ‘Inflammaging and “Garb-aging”’, Trends in Endocrinology & Metabolism, 29(9), pp. 623–633.
Horvath, S. (2013) ‘DNA methylation age of human tissues and cell types’, Genome Biology, 14(10), R115.
Kennedy, B.K. et al. (2014) ‘Geroscience: linking aging to chronic disease’, Cell, 159(4), pp. 709–713.
Levine, M.E. et al. (2018) ‘An epigenetic biomarker of aging for lifespan and healthspan’, Aging (Albany NY), 10(4), pp. 573–591.
López-Otín, C. et al. (2013) ‘The hallmarks of aging’, Cell, 153(6), pp. 1194–1217.
Moffitt, T.E. et al. (2017) ‘Aging trajectories and multimorbidity risk’, The Journals of Gerontology: Series A, 72(2), pp. 175–183.
Organisation for Economic Co-operation and Development (2024) Health at a Glance: Europe 2024. Paris: OECD Publishing.
World Health Organization (2022) Global report on ageing and health. Geneva: WHO.










