Reborne Longevity functions as a fully integrated private hospital rather than a standalone wellness center. The facility occupies a six-floor Marylebone townhouse designed to house diagnostics, specialist consultations, regenerative therapies, and surgical capability within a single coordinated structure.
Unlike fragmented care models, Reborne centralizes oversight. Primary care physicians, metabolic cardiology, nutrition specialists, orthopaedic surgery, regenerative aesthetics, and advanced diagnostics operate within one governance framework.
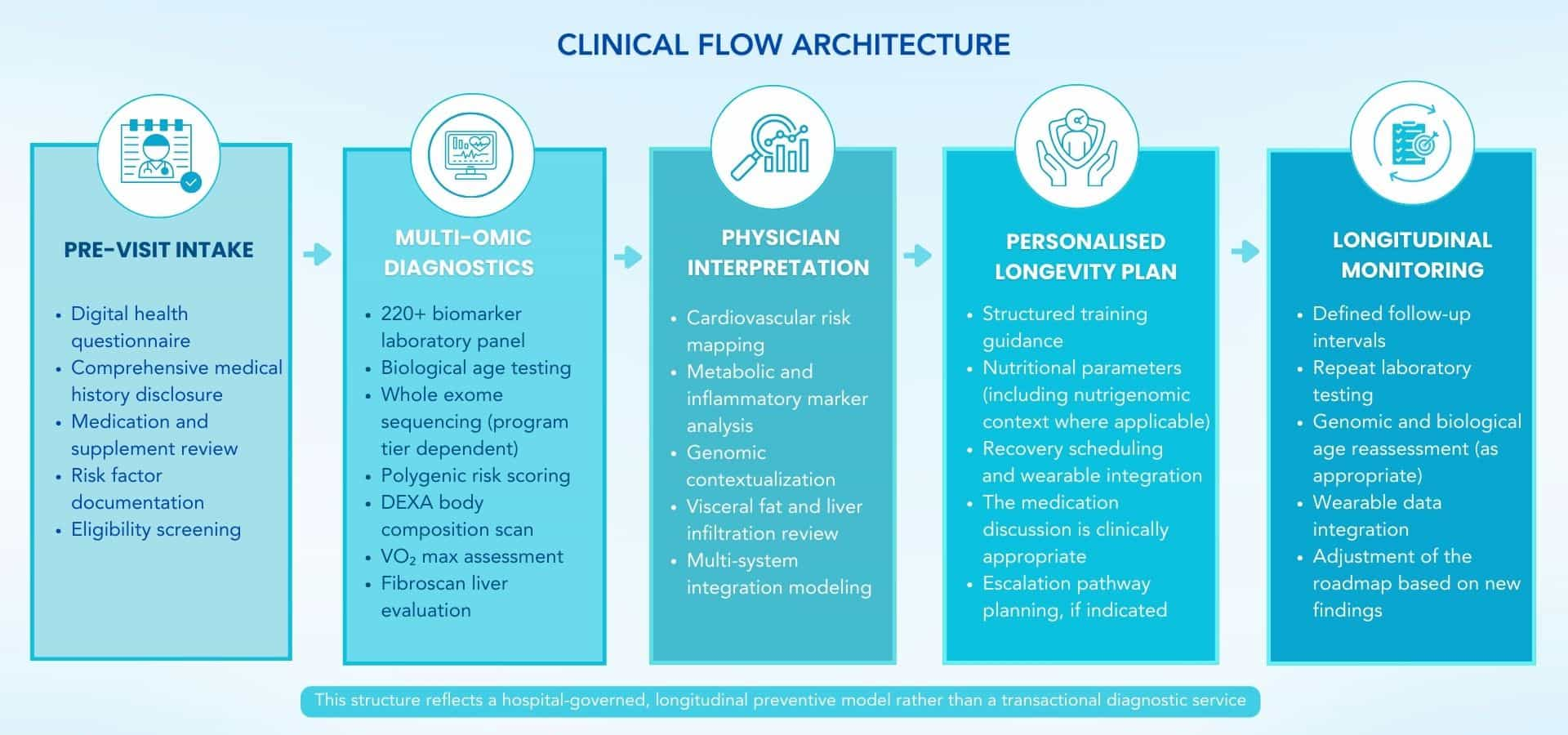
The clinic’s operational flow follows a defined structure:
Intake → Multi-System Diagnostics → Analytical Integration → Structured Plan → Longitudinal Monitoring
Data collection precedes interpretation. Interpretation precedes strategy. Strategy precedes implementation. This sequencing reflects institutional medical governance rather than lifestyle positioning.
Programs are structured across defined time horizons: 3 months, 6–9 months, and 12+ months, depending on complexity and scope.
The hospital setting allows:
- Research-grade wearable integration
- Genomic sequencing
- Advanced imaging, including DEXA and MRI
- Hospital-grade regenerative procedures
All services operate within CQC regulation, ensuring formal medical oversight and accountability.
Executive Time Efficiency
Reborne’s integrated hospital model reduces the coordination burden typically associated with managing multiple specialists across different institutions.
Diagnostics, specialist consultations, imaging, and therapeutic procedures can be consolidated within a single location. Remote monitoring through research-grade wearables and the Reborne Health App supports continuity between in-clinic visits. Many clients combine this with an executive health check for longevity for deeper insights.
For high-performance individuals operating under sustained cognitive or physical demand, this structure provides centralized oversight rather than episodic consultations.
At a Glance – Reborne Longevity
|
Category
|
Details
|
|
Location
|
9 Queen Anne Street, Marylebone, London, UK
|
|
Clinic Type
|
CQC-regulated, clinician-led longevity hospital
|
|
Core Focus
|
Systems biology, biological age analysis, genomic risk mapping
|
|
Typical Program
|
3 to 12+ month structured models
|
|
Diagnostic Depth
|
220+ biomarkers, whole exome sequencing, DEXA, MRI
|
|
Signature Framework
|
P4 Medicine & Systems Biology
|
|
Environment
|
Six-floor integrated private medical facility
|
|
Privacy Level
|
Institutional governance with anonymized lab processing
|
|
Clinical Scope
|
Primary care, diagnostics, regenerative therapies, and surgery
|
Many visitors integrate diagnostic sessions and specialist consultations into existing professional schedules rather than planning extended medical stays.
Marylebone’s central London location supports short, structured visits, particularly for executives already travelling for business. The hospital’s outpatient format allows assessments, imaging, and consultations to be coordinated efficiently within defined appointment windows. You can also explore the best longevity clinics in London to compare similar providers.
Reborne Longevity positions itself as an integrated hospital model designed to reduce fragmentation in modern healthcare. For executives and high-performance individuals, the clinic’s distinction lies in consolidation, systems analysis, and medical governance rather than lifestyle positioning.
Its differentiators are structural rather than emotional.
1. Integrated Hospital Model Under One Roof
Reborne operates as a CQC-regulated private hospital, not a wellness studio or advisory practice. Primary care, advanced diagnostics, genomics, regenerative therapies, and precision surgical services are housed within the same facility.
This eliminates the coordination burden often faced by individuals navigating separate cardiologists, nutritionists, imaging centers, and surgeons across different institutions.
Care remains centralized. Oversight remains physician-led. Documentation remains unified.
For high-performance individuals managing limited time and high responsibility, consolidation reduces friction without compromising governance.
2. Systems Biology Rather Than Symptom Treatment
The clinic applies a Systems Biology approach, evaluating the body as interconnected metabolic, hormonal, neurological, immune, and gut systems.
Rather than addressing fatigue, inflammation, or joint pain in isolation, diagnostics aim to map how system interactions influence broader physiological patterns.
This approach recognizes that chronic disease trajectories often develop over years through networked biological shifts rather than isolated dysfunction.
Mapping precedes modification.
3. Precision Biomarker & Biological Age Analysis
Reborne moves beyond population “normal ranges” and incorporates biological age frameworks such as GrimAge, Phenotypic Age, and KDM-based assessments.
The clinic’s Foundation and Base Camp programs include:
- 220+ biomarker panels
- Biological age clock analysis
- VO₂ max testing
- Grip strength assessment
- DEXA body composition scanning
Biological age acceleration has been associated in research with increased mortality risk. For example, each standard deviation increase in KDM biological age acceleration correlates with approximately a 30% higher risk of all-cause mortality in population studies.
|
🔍 Did You Know?
Grip strength is widely recognized in gerontology research as a reliable functional biomarker. It predicts disability risk and mortality more accurately than chronological age in multiple large cohort studies.
Reborne integrates such markers into structured interpretation rather than treating them as isolated metrics.
|
4. Three-Level Routing Architecture
Reborne applies a structured routing system:
- Level 1 – Remote Monitoring: Continuous tracking via research-grade wearables such as Oura rings and continuous glucose monitors integrated into the Reborne Health App.
- Level 2 – In-Clinic Diagnostics & Treatment: DEXA scans, Fibroscans, full-body MRI, genomic sequencing, and physician consultations.
- Level 3 – Individualised Scientific Studies: For complex cases, deeper phenotyping supported by AI-driven data integration and specialist networks.
This tiered architecture allows escalation based on complexity rather than applying uniform protocols to all individuals.
5. Advanced Regenerative Interventions Within Governance
Where clinically appropriate, the hospital offers procedures such as:
- Therapeutic Plasma Exchange (TPE)
- EBO2 blood optimization
- Arthrosamid for knee osteoarthritis
- Precision orthopaedic regenerative procedures
TPE has been studied for its potential to reduce inflammatory burden and for the “peripheral sink” mechanism explored in Alzheimer’s research contexts.
These interventions are delivered within a regulated hospital environment rather than a retail wellness setting. For a broader comparison, see the best longevity clinics in the UK.
The clinic does not claim disease reversal. Procedures are positioned as medically governed interventions requiring specialist oversight.
6. Elimination of Fragmentation
High-performance individuals often face healthcare fragmentation: multiple providers, uncoordinated diagnostics, repeated histories, and conflicting advice.
Reborne’s single-source integration model centralizes:
- Diagnostics
- Genomics
- Nutrition
- Metabolic cardiology
- Orthopaedics
- Regenerative aesthetics
- Primary care
This structure aims to reduce friction and consolidate accountability.
Reborne Longevity positions its clinical model around healthspan expansion rather than episodic disease treatment. The objective is to identify measurable biological shifts early, before conventional diagnostic thresholds are crossed, and translate findings into structured longitudinal planning.
In England, males spend approximately 61.5 years and females 61.9 years in good health. This measurable gap between lifespan and years lived in optimal functional capacity informs the clinic’s preventive orientation.
The model does not frame aging as reversed or cured. It approaches aging as a modifiable biological process influenced by metabolic, inflammatory, genomic, and behavioral variables. Diagnostics map these variables; they do not determine future outcomes with certainty.
Programs are structured across defined time horizons: 3 months, 6–9 months, and 12+ months, depending on complexity and scope.
Clinical Purpose
Reborne’s clinical intent centers on three structural pillars:
- Early Risk Identification: Moving beyond population “normal ranges” to identify emerging deviations in biomarkers such as HbA1c, inflammatory markers, and lipid parameters before disease thresholds are formally reached.
- System-Level Mapping: Evaluating how metabolic, hormonal, neurological, immune, and gut systems interact rather than isolating symptoms.
- Long-Term Health Governance: Establishing a structured roadmap supported by repeat diagnostics, wearable integration, and defined review intervals.
Population-level research suggests that improving diet quality in midlife is associated with extended life expectancy. Observational studies also show that combining anti-inflammatory dietary patterns with moderate physical activity and adequate sleep correlates with lower all-cause mortality risk.
Who This Clinic Is Designed For
Reborne Longevity is structured for adults operating under sustained cognitive or physical demand who require consolidated oversight rather than fragmented consultations.
Typical profiles include:
- Chief executives and senior corporate leaders
- Founders and entrepreneurs
- Institutional investors
- Professional and endurance athletes
- Individuals managing complex metabolic or inflammatory conditions under physician supervision
Many participants integrate programs into ongoing professional schedules rather than residential stays. The hospital environment supports discretion, coordinated care, and centralized oversight.
Focus Areas
|
Focus Area
|
What This Means in Practice
|
|
Medical Discipline
|
Longevity medicine is grounded in systems biology and genomic analysis
|
|
Core Biological Systems
|
Metabolic, hormonal, neurological, immune, and gut health
|
|
Environment
|
CQC-regulated integrated private hospital
|
|
Program Structure
|
Foundation (3 months), Base Camp (6–9 months), Bespoke (12+ months)
|
|
Lifestyle as Medicine
|
Nutrigenomics, VO₂ max testing, grip strength, sleep, and glucose monitoring
|
|
Privacy
|
Anonymized lab processing with accredited laboratories
|
|
Long-Term Strategy
|
Repeat biomarker testing, biological age tracking, longitudinal oversight
|
Reborne Longevity applies a P4 Medicine framework, Predictive, Preventive, Personalised, and Participatory, within a regulated hospital environment. The philosophy shifts focus from reactive disease treatment toward earlier biological mapping.
Traditional healthcare models often intervene once diagnostic thresholds are crossed. Reborne’s model seeks to identify measurable deviations before those thresholds are reached, using biomarker panels, genomic sequencing, and biological age analytics.
The clinic integrates Systems Biology principles, viewing the body as a network of interconnected metabolic, hormonal, neurological, immune, and gut systems. Rather than isolating symptoms, interpretation evaluates how system-level interactions influence overall physiological trajectory.
Diagnostics are interpreted under physician supervision. Data dashboards or wearable outputs are not positioned as standalone decision tools.
Predictive & Biological Age Frameworks
Reborne incorporates validated biological age methodologies, including:
- GrimAge epigenetic clock testing
- Klemera–Doubal Method (KDM) biological age modeling
- Phenotypic Age algorithms
- Grip strength as a functional aging biomarker
- VO₂ max as a cardiorespiratory longevity marker
Research suggests that biological age acceleration, particularly through KDM modeling, correlates with increased all-cause mortality risk. In population studies, increases in biological age acceleration have been associated with elevated all-cause mortality risk, though these associations do not determine individual outcomes.
These models are used to contextualize physiological status relative to functional aging markers. They do not determine individual lifespan.
|
🔍 Did You Know?
Expert consensus panels have identified biomarkers such as IGF-1, IL-6, high-sensitivity C-reactive protein (hsCRP), and grip strength as reliable indicators associated with aging trajectories in clinical research.
Reborne integrates such markers into a structured analytical review rather than relying on chronological age alone.
|
Systems-Level Interpretation
The clinic’s Analytical Center functions as a centralized integration hub. It combines:
- 220+ biomarker panels
- Whole exome sequencing
- Polygenic risk scoring
- Gut microbiome analysis
- Continuous glucose monitoring
- Research-grade wearable tracking (e.g., Oura ring integration)
AI-assisted analysis supports pattern recognition across metabolic, inflammatory, hormonal, and genomic domains.
This approach aims to deeply phenotype an individual’s biological state rather than rely on isolated laboratory results.
Lifestyle as a Clinical Variable
Reborne incorporates nutrigenomics and functional medicine principles into interpretation.
Examples include:
- Tailored dietary guidance based on genetic variants (e.g., MTHFR, APOE, COMT)
- Continuous glucose monitoring to evaluate glycemic variability
- VO₂ max and activity threshold assessment
- Grip strength testing
- Sleep pattern analysis via wearable integration
Research suggests that higher physical activity levels, including ≥ 3000 MET-minutes per week, are associated with deceleration in biological aging markers in certain cohorts. These findings are observational and do not prescribe universal thresholds. Improving sleep quality for recovery is a key part of long-term health strategy.
|
🔍 Did You Know?
Medical-grade DEXA scanning is one of the most precise methods available to quantify visceral adipose tissue, the metabolically active fat around internal organs that correlates with cardiometabolic risk patterns.
Lifestyle inputs are framed as modifiable variables within physician-guided oversight rather than generalized wellness recommendations.
|
Reborne Longevity applies a diagnostics-first architecture designed to establish a multi-system biological baseline before structured planning begins. Assessment precedes strategy. Strategy precedes implementation.
The clinic’s diagnostic framework integrates molecular, metabolic, genomic, and functional data within a hospital-regulated setting. Tools are selected to identify measurable physiological patterns associated with long-term risk trajectories rather than acute symptom management.
No single marker is treated as determinative. Interpretation occurs within a broader systems context under physician supervision.
Diagnostic Assessment Includes
Reborne’s core programs incorporate layered diagnostic depth depending on complexity and program tier.
- Multi-System Biomarker Panels (220+ Markers): Comprehensive laboratory panels assessing inflammatory markers, lipid profiles, hormonal status, glycemic control, metabolic indicators, and organ function metrics.
- Biological Age Analysis: GrimAge, KDM, and Phenotypic Age modeling to contextualize functional aging relative to population benchmarks.
- Whole Exome Sequencing: Genomic sequencing to evaluate inherited risk patterns across multiple disease categories.
- Polygenic Risk Scores: Risk stratification modeling for conditions such as Alzheimer’s disease, coronary artery disease, and other major chronic conditions.
- DEXA Body Composition Analysis: Medical-grade quantification of visceral adipose tissue (VAT), lean mass distribution, and bone density.
- Full-Body MRI (Bespoke Tier): Comprehensive imaging for structural and internal assessment when clinically indicated.
- Fibroscan & Liver Assessment: Evaluation of hepatic fat and fibrosis patterns.
- Continuous Glucose Monitoring (CGM): Two-week glucose variability tracking to assess metabolic flexibility.
- Cardiorespiratory Fitness Testing (VO₂ Max): Measurement of oxygen utilization capacity as a marker associated with functional longevity.
- Grip Strength Testing: Functional strength assessment is linked in research to disability and mortality risk patterns.
Diagnostics are integrated into a 60–80 page personalized health roadmap within flagship programs.
|
🔍 Did You Know?
Visceral adipose tissue cannot be accurately measured using BMI or standard scales. Medical-grade DEXA scanning provides quantification of this metabolically active fat, which is associated with cardiometabolic risk patterns in clinical research.
|
Three-Level Clinical Routing
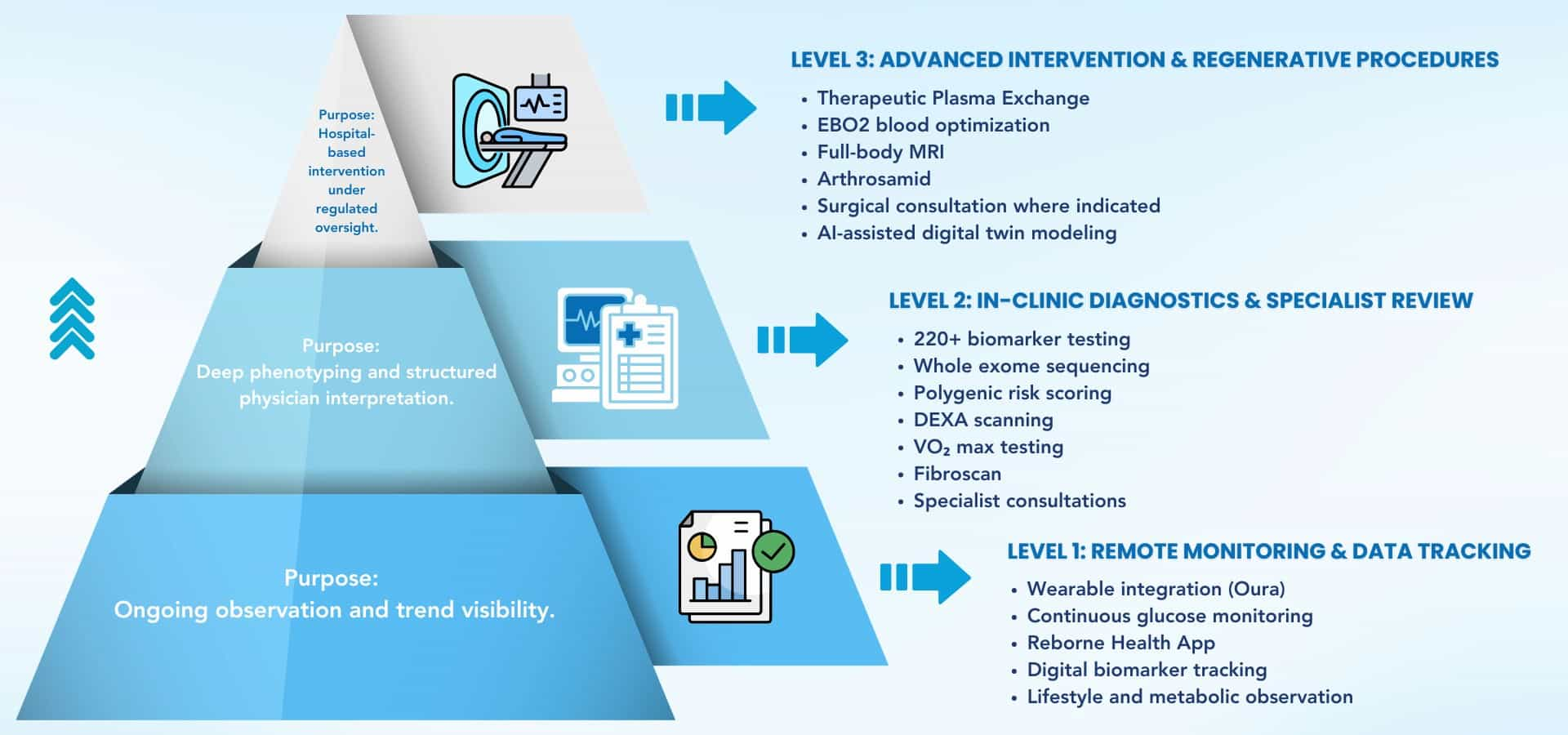
Reborne applies a structured routing architecture based on complexity.
- Level 1 – Remote Monitoring: Wearable integration (e.g., Oura ring), CGM data, and digital tracking via the Reborne Health App support longitudinal observation between visits.
- Level 2 – In-Clinic Diagnostics & Treatment: Advanced imaging, genomic sequencing, and physician consultations are conducted on-site within the hospital environment.
- Level 3 – Individualised Scientific Studies: For complex or rare conditions, deeper phenotyping and AI-assisted modeling are applied to generate a “digital twin” framework for individualized analysis.
Escalation between levels is determined by clinical complexity rather than standardized packages.
Regenerative & Hospital-Grade Interventions
Where clinically appropriate, Reborne offers advanced procedures delivered within regulated hospital governance.
These may include:
- Therapeutic Plasma Exchange (TPE) – A hospital-based procedure designed to remove inflammatory mediators and pathogenic proteins from plasma. TPE has been studied for its potential role in immune burden reduction and the “peripheral sink” mechanism explored in Alzheimer’s research contexts. It is not positioned as a cure.
- EBO2 Blood Optimization – A medical-grade oxygenation and ozone-based process aimed at supporting immunological balance under supervision.
- Arthrosamid – A non-surgical hydrogel implant used in knee osteoarthritis management, providing long-term joint cushioning in selected cases.
Such interventions are delivered under CQC regulation with specialist oversight. They are not presented as anti-aging reversals or guaranteed disease prevention strategies. Many programs also focus on how to improve immune resilience for longevity.
Reborne Longevity differentiates itself through structural integration rather than service breadth. Its strengths lie in consolidation, systems analysis, and regulated delivery within a hospital framework.
The clinic’s positioning centers on reducing fragmentation while increasing diagnostic precision.
Key Medical Strength 1 – Single-Source Integrated Hospital Model
Reborne operates as an integrated private hospital rather than a distributed referral network. Primary care, genomics, advanced diagnostics, regenerative therapies, metabolic cardiology, orthopaedics, and surgical capability are centralized within one six-floor Marylebone facility.
For high-performance individuals, healthcare fragmentation often results in repeated histories, duplicated diagnostics, and conflicting interpretations across separate providers.
Reborne’s structure consolidates:
- Diagnostic testing
- Specialist consultations
- Imaging
- Regenerative procedures
- Surgical services
This reduces coordination burden while maintaining institutional governance under CQC regulation.
Care remains physician-led and centrally documented.
Key Medical Strength 2 – Analytical Center & Precision Data Translation
The clinic’s Analytical Center functions as a centralized integration hub.
It combines:
- 220+ biomarkers
- Whole exome sequencing
- Polygenic risk scoring
- Biological age modeling
- Gut microbiome analysis
- Continuous glucose monitoring
- Research-grade wearable data
AI-assisted analysis supports multi-omic pattern recognition across metabolic, inflammatory, hormonal, and genomic domains.
Rather than delivering isolated laboratory results, findings are synthesized into a structured 60–80 page personal health roadmap.
The emphasis is on interpretation, not raw data volume.
|
🔍 Did You Know?
Each standard deviation increase in KDM biological age acceleration has been associated In population-level studies, increases in KDM biological age acceleration have been associated with elevated all-cause mortality risk, though these associations do not determine individual prognosis. Biological age models are predictive tools, not determinative forecasts.
Reborne applies such models as contextual frameworks within physician-led oversight.
|
Key Medical Strength 3 – Systems Biology Root-Cause Mapping
The clinic evaluates interconnected biological systems rather than isolated symptoms.
For example:
- Fatigue may involve metabolic flexibility, micronutrient status, hormonal signaling, and inflammatory burden.
- Chronic inflammation may reflect gut permeability, immune dysregulation, and visceral adiposity patterns.
By mapping system interactions, the clinic seeks to identify upstream drivers rather than only managing downstream manifestations.
This approach aligns with its P4 Medicine framework.
Key Medical Strength 4 – Regenerative Procedures Within Governance
Reborne offers hospital-grade procedures such as:
- Therapeutic Plasma Exchange (TPE)
- EBO2 blood optimization
- Arthrosamid for knee osteoarthritis
- Precision orthopaedic regenerative techniques
TPE has been studied for immune burden reduction and explored in Alzheimer’s research for its potential “peripheral sink” mechanism related to amyloid-β redistribution. These studies remain evolving.
All regenerative procedures are delivered within a regulated hospital setting with specialist supervision.
The clinic does not position these interventions as cures or age reversal mechanisms. They are presented as medically governed procedures within defined clinical contexts.
The following examples reflect reported experiences and publicly described cases associated with the clinic’s integrated model. They illustrate how structured diagnostics informed clinical planning. They do not represent guaranteed outcomes, and individual results vary.
Outcome 1 – System-Level Identification of Chronic Inflammation
Before:
An individual experiencing persistent bloating and long-standing inflammatory skin symptoms had previously pursued symptom-focused treatments without durable resolution.
After:
Through multi-system assessment, including gut microbiome analysis, inflammatory markers, and metabolic profiling, interpretation focused on internal systemic drivers rather than surface symptoms. A structured plan addressed nutritional, inflammatory, and metabolic contributors under physician supervision.
The reported outcome was improved symptom control and greater clarity regarding root biological contributors.
Source:
Publicly described patient case narratives associated with clinic programs.
Outcome 2 – Elite Athletic Recovery & Monitoring
Before:
An endurance athlete managing sustained training loads sought structured oversight to better understand recovery variability and metabolic strain.
After:
Integration of biological age markers, continuous glucose monitoring, VO₂ max testing, and IV-based recovery protocols enabled longitudinal monitoring under physician oversight.
The reported experience emphasized improved insight into recovery patterns rather than performance enhancement claims.
Source:
Executive and athletic case examples are publicly described in clinic-related materials.
Outcome 3 – Metabolic & Cardiovascular Risk Mapping
Before:
A high-performance executive with no overt symptoms sought preventive assessment.
After:
Comprehensive biomarker panels, DEXA-based visceral fat quantification, and polygenic risk scoring identified early-stage metabolic and cardiovascular risk markers that were not previously tracked.
The outcome centered on awareness and structured planning rather than acute disease treatment.
Source:
Preventive case structures are described within longevity program materials.
|
⚠️ Editorial Note
These outcomes reflect individual experiences reported in publicly available materials. They do not constitute medical claims or guarantees. Diagnostics identify measurable physiological patterns at a given time. Individual responses vary based on genetics, environment, medical history, and adherence to physician guidance. Participation does not replace consultation with a primary physician.
|
Reborne Longevity structures its services across defined program tiers based on diagnostic depth and monitoring duration. Programs are differentiated by complexity, genomic integration, imaging scope, and longitudinal oversight.
They are not positioned as curative pathways. Each program reflects a structured medical assessment followed by physician interpretation and monitored follow-up.
Foundation (£4,500) – 3 Months
Format:
Three-month structured baseline assessment.
Clinical Intent:
Establish a multi-system biological baseline and functional aging profile.
Included Components:
- 220+ biomarker laboratory panel
- GrimAge biological age testing
- VO₂ max assessment
- Grip strength testing
- DEXA body composition analysis
- Physician consultation and structured review
The Foundation program establishes a measurable baseline across metabolic, inflammatory, hormonal, and cardiovascular domains. Findings are consolidated into a structured health roadmap.
The £4,500 pricing reflects diagnostic scope and physician-led interpretation rather than guaranteed outcome improvement.
This tier is suitable for individuals seeking structured biological mapping without immediate genomic sequencing or advanced imaging.
Base Camp (£14,500) – 6 to 9 Months
Format:
Six to nine-month structured program integrating genomic and multi-system analysis.
Clinical Intent:
Expand baseline diagnostics into genomic risk modeling and longitudinal metabolic tracking.
Included Components:
- All Foundation components
- Whole exome sequencing
- Polygenic risk scoring (8+ major diseases, including Alzheimer’s and coronary artery disease)
- Gut microbiome analysis
- Continuous glucose monitoring
- Extended physician consultations
- Structured follow-up testing
The Base Camp program integrates genetic risk architecture with metabolic and inflammatory profiling. The emphasis is on contextualizing inherited predisposition alongside modifiable biological variables.
The £14,500 pricing reflects genomic analysis, expanded diagnostics, and extended oversight across the 6–9 month period.
This program is designed for individuals seeking deeper precision in risk modeling and multi-omic integration.
Bespoke (£25,000–£50,000+) – 12+ Months
Format:
Twelve-month or longer individualized commitment for complex or high-level oversight.
Clinical Intent:
Provide longitudinal governance for individuals with complex conditions, high-performance demands, or advanced diagnostic requirements.
Included Components:
- Full-body MRI
- Unlimited specialist consultations
- Priority access to regenerative therapies
- Dedicated care coordinator
- Advanced diagnostics escalation where indicated
- AI-assisted deep phenotyping
The Bespoke tier reflects full-spectrum integration within the hospital environment, including surgical access and specialist-led regenerative procedures when clinically appropriate.
Pricing begins at £25,000 and may exceed £50,000 depending on scope, imaging requirements, and specialist involvement.
This tier is structured for sustained oversight rather than single-event assessment.
Programs are structured around defined review cycles. Diagnostic findings are interpreted under physician supervision. Monitoring supports pattern tracking over time rather than static measurement.
Reborne Longevity operates from a six-floor Marylebone townhouse functioning as a CQC-regulated private hospital. The facility integrates diagnostics, consultation suites, imaging capability, regenerative procedures, and surgical infrastructure within a single governed environment.
It is not structured as a residential retreat. It functions as an outpatient medical hospital with defined program pathways and specialist oversight.
Named Technologies & Diagnostic Platforms
Reborne incorporates the following tools within its clinical architecture:
- Multi-System Biomarker Panels (220+ Markers): Comprehensive laboratory testing covering metabolic, inflammatory, hormonal, cardiovascular, and organ-function domains.
- Whole Exome Sequencing: Genomic analysis evaluating inherited variants across protein-coding regions.
- Polygenic Risk Scoring: Risk stratification modeling for major chronic disease categories.
- Biological Age Clocks: GrimAge, KDM, and Phenotypic Age algorithms for functional aging contextualization.
- DEXA Scanning: Medical-grade body composition analysis quantifying visceral adipose tissue and lean mass distribution.
- Full-Body MRI (Bespoke Tier): Comprehensive imaging capability when clinically indicated.
- Fibroscan: Assessment of liver fat and fibrosis patterns.
- Continuous Glucose Monitoring (CGM): Two-week metabolic flexibility tracking.
- VO₂ Max Testing: Cardiorespiratory capacity assessment associated with functional longevity metrics.
- Grip Strength Measurement: A functional aging biomarker associated with disability and mortality risk in population research.
All diagnostic findings are interpreted collectively under physician supervision.
Advanced Regenerative & Procedural Services
Where clinically appropriate, the hospital offers:
- Therapeutic Plasma Exchange (TPE): A hospital-based plasma filtration procedure designed to remove inflammatory mediators and circulating proteins. TPE has been studied in immune modulation contexts and explored in Alzheimer’s research through the “peripheral sink” hypothesis. It is not positioned as curative.
- EBO2 Blood Optimization: A medical-grade oxygenation and ozone-based process aimed at supporting immunological balance under supervision.
- Arthrosamid: A non-surgical hydrogel implant used in selected knee osteoarthritis cases, designed to provide joint cushioning for extended durations.
- Regenerative Orthopaedic Techniques: Specialist-led knee preservation and biologic therapies within surgical governance.
All procedures are delivered within a regulated hospital framework under specialist oversight.
Analytical Center & Data Integration

The clinic’s Analytical Center functions as its central integration hub.
It synthesizes:
- Multi-omic laboratory data
- Genomic sequencing
- Biological age modeling
- Microbiome profiling
- Wearable tracking (e.g., Oura integration)
- Continuous glucose monitoring
AI-assisted systems support pattern recognition across interconnected biological domains.
Data remains physician-interpreted. Machine learning assists integration but does not replace clinical judgment.
Governance, Privacy & Laboratory Standards
Reborne operates under the Care Quality Commission (CQC) regulation. Laboratory samples are processed using anonymized patient reference numbers rather than names.
The clinic partners exclusively with laboratories accredited under standards such as:
This structure supports genomic privacy, traceability, and institutional accountability.
Architecture & Environment
The facility is designed to reduce patient stress while maintaining clinical discipline. The interior includes consultation lounges, infusion suites, and surgical facilities integrated within the townhouse structure.
While often described as refined or hospitality-oriented, the environment operates within a regulated hospital framework rather than a spa model.
Care remains appointment-based and medically governed.
Reborne Longevity operates within a private hospital model in central London. Pricing reflects diagnostic depth, genomic integration, imaging capability, specialist oversight, and longitudinal monitoring architecture.
Fees are not performance-based and do not guarantee biological outcomes. Suitability and scope are confirmed following intake review and physician assessment.
Pricing
|
Category
|
Details
|
|
Clinic Positioning
|
CQC-regulated private hospital focused on preventive longevity and multi-omic diagnostics
|
|
Stay Length
|
Outpatient; duration depends on program tier
|
|
Entry Pricing
|
£4,500 (Foundation – 3 months)
|
|
Mid-Tier Program
|
£14,500 (Base Camp – 6 to 9 months)
|
|
Advanced Tier
|
£25,000–£50,000+ (Bespoke – 12+ months)
|
|
What’s Included
|
Multi-system diagnostics, physician consultations, structured roadmap
|
|
Additional Costs
|
Advanced imaging, regenerative procedures, and surgical interventions where indicated
|
|
Program Structure
|
Intake → Diagnostics → Physician Interpretation → Roadmap → Longitudinal Monitoring
|
|
Clinical Principle
|
Risk identification before symptomatic thresholds
|
Pricing reflects access to structured medical oversight and hospital-based infrastructure rather than guaranteed outcomes.
How Programs Are Structured
All programs follow a defined governance sequence:
1. Pre-Visit Phase
- Digital intake documentation
- Medical history review
- Medication disclosure
- Eligibility screening
2. Diagnostic Phase
- Multi-system laboratory testing
- Imaging (DEXA, MRI, where applicable)
- Genomic sequencing (Base Camp & Bespoke tiers)
- Biological age testing
- Functional assessments (VO₂ max, grip strength)
3. Physician Interpretation Phase
- Cardiovascular risk mapping
- Metabolic and inflammatory analysis
- Genomic contextualization
- Structured discussion of findings
4. Planning & Monitoring Phase
- Written longevity roadmap
- Structured follow-up consultations
- Repeat laboratory testing at defined intervals
- Escalation to advanced procedures where clinically indicated
Evaluation precedes strategy. Strategy precedes implementation. Monitoring occurs at defined intervals. These structured programs are similar to executive longevity testing packages designed for high performers.
Length of Stay
Reborne operates exclusively as an outpatient hospital.
Duration varies by program:
- Foundation: Diagnostic sessions across initial visits within a 3-month period
- Base Camp: Expanded diagnostics and follow-up consultations over 6–9 months
- Bespoke: Longitudinal oversight extending 12 months or longer
There is no mandatory residential admission. Surgical or procedural interventions, when performed, follow standard hospital scheduling protocols.
Appointments are integrated into professional schedules rather than immersive retreats.
Reborne Longevity operates from a six-floor CQC-regulated private hospital in Marylebone, central London. Visits are typically integrated into professional travel schedules rather than planned as extended medical stays.
All attendance is appointment-based. There is no residential program requirement.
Recommended Visit Duration
Visit duration depends on the selected program tier and diagnostic scope.
- Foundation (3 months): Initial diagnostic sessions scheduled across early visits, followed by structured review.
- Base Camp (6–9 months): Expanded diagnostics and genomic testing, with periodic consultations during the monitoring period.
- Bespoke (12+ months): Ongoing oversight, specialist coordination, and advanced imaging scheduled as clinically indicated.
Procedural appointments such as MRI, Fibroscan, TPE, or orthopaedic interventions follow hospital scheduling protocols.
There is no mandatory overnight admission unless a surgical procedure requires standard post-operative observation.
Follow-up consultations may occur in person or remotely, depending on the physician's discretion and patient logistics.
How to Reach the Clinic
City: London, United Kingdom
Area: Marylebone
Regulatory Status: CQC-regulated private hospital
Nearest Airport: London Heathrow Airport (LHR)
Typical Transfer Time: Approximately 45–60 minutes by car, depending on traffic conditions.
Transport Options:
- Licensed taxi services
- Ride-share platforms
- London Underground
- National rail connections
- Private chauffeur services
🔗 Find best flights to London
🔗 Find car rentals in London
Links are provided for travel planning convenience only.
Accommodation & Stay Planning
Reborne Longevity does not operate on-site accommodation.
Visitors typically stay at:
- Central London business hotels
- Serviced apartments in Marylebone
- Boutique hotels within walking distance
Accommodation arrangements are independent of hospital operations.
🔗 Explore nearby hotels & apartments
What to Bring
Participants are generally advised to bring:
- Government-issued identification
- Prior medical documentation (if available)
- Current medication list
- Comfortable clothing suitable for exercise testing
- Any wearable devices currently used for health tracking
Additional documentation requirements are communicated during intake review.
Reborne Longevity has been positioned within the emerging longevity medicine sector as a hospital-based, data-integrated model combining diagnostics, genomics, and regenerative medicine under one regulatory structure.
Public discussions surrounding the clinic focus on its multi-omic integration, hospital governance, and emphasis on systemic root-cause evaluation rather than isolated biomarker optimization.
Longevity medicine remains a developing scientific field. Biomarkers often reflect risk associations rather than deterministic outcomes. Observational research dominates much of the discipline due to the impracticality of lifespan-length clinical trials.
Reborne’s positioning emphasizes structure and integration over outcome guarantees.
What Patients Commonly Report
Based on publicly described case narratives and sector commentary, recurring themes include:
- Greater visibility into previously unmeasured biological systems
- Identification of inflammatory or metabolic contributors not addressed in symptom-focused care
- Appreciation for genomic risk contextualization
- Clarity in understanding how multiple systems interact
- Structured follow-up rather than one-time data reporting
Reports frequently highlight the Analytical Center’s ability to consolidate laboratory, genomic, microbiome, and wearable data into a unified interpretation framework.
These experiences reflect subjective accounts. They do not represent guaranteed clinical outcomes.
Professional & Industry Positioning
Reborne Longevity is distinguished by:
- CQC-regulated private hospital status
- Integration of surgical, regenerative, and diagnostic services under one roof
- Use of whole-exome sequencing and polygenic risk scoring
- Inclusion of biological age algorithms (e.g., GrimAge)
- Multi-omic analytical architecture
Sector commentary often references its hospital-based infrastructure as a differentiator from boutique wellness clinics.
Operational scale, technological integration, or media visibility do not equate to validated long-term lifespan outcomes. The broader field of preventive geroscience continues to evolve.
Reborne Longevity operates within the evolving field of preventive geroscience, combining hospital-based governance with multi-omic diagnostics and longitudinal monitoring. Its positioning differs from lifestyle-oriented longevity centers by embedding genomic sequencing, advanced imaging, and regenerative procedures within a regulated private hospital framework.
The broader longevity sector remains scientifically transitional. Many biomarkers associated with aging and chronic disease are supported by observational correlations rather than definitive lifespan trials. Biological age algorithms and polygenic risk scores offer probabilistic insight, not deterministic forecasts. Surrogate markers are often used because decades-long outcome studies are impractical.
Within these constraints, Reborne’s model emphasizes structured interpretation over technological novelty. Diagnostics precede strategy. Strategy is reviewed longitudinally. Regenerative procedures are delivered under specialist supervision rather than experimental positioning. This reflects trends seen across the best longevity clinics in Europe.
For executives who approach health as governance rather than episodic repair, the clinic offers system-level visibility and scheduled reassessment within acknowledged scientific limits. The value lies in integration and oversight, not in outcome guarantees.
Is Reborne Longevity a medical hospital or a wellness clinic?
Reborne operates as a Care Quality Commission (CQC)-regulated private hospital in central London. It is structured around physician-led diagnostics, genomic sequencing, imaging, and regulated procedures.
It is not positioned as a spa, retreat, or lifestyle optimization center. All assessments and interventions occur within a hospital governance framework.
Who is Reborne Longevity designed for?
The clinic primarily serves executives, founders, investors, professional athletes, and individuals operating under sustained cognitive or performance demand.
It is structured for those seeking systematic biological evaluation, genomic risk modeling, and longitudinal oversight rather than acute disease treatment.
Are programs personalised?
Yes. Interpretation is individualized based on biomarker data, genomic sequencing, imaging findings, medical history, and physician review.
Programs are structured but not protocol-driven without prior assessment. Recommendations follow diagnostic interpretation rather than precede it.
Does Reborne treat chronic diseases such as diabetes, heart disease, or cancer?
Reborne focuses on preventive diagnostics, risk mapping, and regenerative procedures within a hospital setting.
It does not replace specialist disease management programs. Individuals with established medical conditions should continue working with their primary physicians or consultants.
Are genomic and biological age tests definitive?
No. Genomic sequencing and biological age algorithms provide probabilistic insight based on population-level data.
They identify risk associations rather than certainties and must be interpreted within full clinical context.
Is privacy maintained?
Yes. The hospital operates under CQC regulation and established UK medical confidentiality standards.
Laboratory samples are anonymized using reference identifiers. Data handling follows regulated governance procedures.
Can I continue working during the program?
Yes. Reborne functions as an outpatient hospital. Most diagnostics and consultations are appointment-based and can be integrated into existing professional schedules.
Certain procedures may require recovery time consistent with standard medical practice.
Does participation guarantee prevention or lifespan extension?
No. Diagnostics identify measurable physiological patterns at a given time. They do not guarantee disease avoidance, reversal, or extended lifespan.
Longevity medicine remains an evolving field supported largely by observational research.
How should value be evaluated relative to cost?
Evaluation may consider:
- Depth of multi-system biomarker testing (220+ markers)
- Whole exome sequencing and polygenic risk scoring
- Biological age modeling
- Imaging capability including full-body MRI
- Regulated hospital infrastructure
- Longitudinal physician oversight
Pricing reflects diagnostic architecture and clinical governance rather than promised outcomes.
A Strategic Pause That Protects the Years Ahead
High-performance careers rarely decline suddenly. They erode incrementally through compressed recovery cycles, sustained cognitive load, irregular sleep, metabolic drift, and unmeasured inflammation. The effect is rarely visible in a single quarter. It accumulates over the years.
Reborne Longevity positions itself within this long-arc perspective.
Its model does not promise reversal of aging or immunity from disease. Instead, it offers structured visibility into biological systems that often remain unmeasured until symptoms appear. Genomic sequencing, multi-omic biomarker panels, imaging, and biological age modeling are consolidated within a regulated hospital framework and interpreted under physician supervision.
The broader longevity sector continues to evolve. Many biomarkers are associative rather than causative. Polygenic risk scores provide probability ranges, not certainty. Biological age clocks estimate trajectory, not destiny.
Within these constraints, structured oversight may provide clarity.
For executives who approach health as governance rather than episodic repair, the value lies in disciplined evaluation, contextual interpretation, and periodic reassessment. Measurement does not guarantee outcome but the absence of measurement guarantees uncertainty.
Reborne offers structure, not promise.
👉 View Longevity Program
↩ Return to ExtendMy.Life
↑ Back to Top
Disclaimer
This clinic profile is provided for informational and editorial purposes only. It does not constitute medical advice, diagnosis, treatment recommendation, or endorsement. No doctor–patient relationship is created through this content.
Reborne Longevity operates as a CQC-regulated private hospital offering preventive diagnostics, genomic analysis, imaging, and regulated medical procedures under physician supervision. The information presented here describes clinical structure, governance, and publicly referenced service architecture. It is not intended to guide individual healthcare decisions.
Diagnostic tools such as multi-system biomarker panels, whole exome sequencing, polygenic risk scoring, biological age algorithms, full-body MRI, DEXA scanning, continuous glucose monitoring, and regenerative procedures identify measurable physiological or probabilistic risk patterns at a specific point in time. These findings do not predict certainty of disease, guarantee prevention, reverse aging, or determine lifespan.
Longevity medicine is an evolving scientific discipline. Many associations between biomarkers and long-term outcomes are observational rather than causative. Surrogate markers are frequently used because definitive lifespan trials are impractical. Individual biological responses vary based on genetics, medical history, environment, and adherence to physician guidance.
Individuals with chronic conditions, including cardiovascular disease, diabetes, autoimmune disorders, neurological conditions, or active cancer, should consult their personal physician or specialist before participating in any new diagnostic or medical program.
All healthcare decisions should be made in consultation with a qualified licensed medical professional who understands the individual’s complete medical history.
ExtendMy.Life does not guarantee clinical outcomes and assumes no responsibility for medical decisions made based on this informational profile.
References
Benjamin, E.J., Muntner, P., Alonso, A., Bittencourt, M.S., Callaway, C.W., Carson, A.P., Chamberlain, A.M., Chang, A.R., Cheng, S., Das, S.R. and Delling, F.N. (2019) ‘Heart disease and stroke statistics—2019 update: A report from the American Heart Association’, Circulation, 139(10), pp. e56–e528.
Belsky, D.W., Caspi, A., Arseneault, L., et al. (2015) ‘Quantification of biological aging in young adults’, Proceedings of the National Academy of Sciences, 112(30), pp. E4104–E4110.
Franceschi, C. and Campisi, J. (2014) ‘Chronic inflammation (inflammaging) and its potential contribution to age-associated diseases’, The Journals of Gerontology: Series A, 69(Suppl 1), pp. S4–S9.
Horvath, S. (2013) ‘DNA methylation age of human tissues and cell types’, Genome Biology, 14(10), p. R115.
Levine, M.E., Lu, A.T., Quach, A., et al. (2018) ‘An epigenetic biomarker of aging for lifespan and healthspan’, Aging (Albany NY), 10(4), pp. 573–591.
Levine, M.E., Lu, A.T., Chen, B.H., et al. (2019) ‘DNA methylation GrimAge strongly predicts lifespan and healthspan’, Aging (Albany NY), 11(2), pp. 303–327.
Libby, P. (2002) ‘Inflammation in atherosclerosis’, Nature, 420(6917), pp. 868–874.
Loos, R.J.F. (2012) ‘Genetic determinants of common obesity and their value in prediction’, Best Practice & Research Clinical Endocrinology & Metabolism, 26(2), pp. 211–226.
Siegel, R.L., Miller, K.D., Wagle, N.S. and Jemal, A. (2023) ‘Cancer statistics, 2023’, CA: A Cancer Journal for Clinicians, 73(1), pp. 17–48.
Torkamani, A., Wineinger, N.E. and Topol, E.J. (2018) ‘The personal and clinical utility of polygenic risk scores’, Nature Reviews Genetics, 19(9), pp. 581–590.
UK Biobank (2015) UK Biobank: Protocol for a large-scale prospective epidemiological resource. Stockport: UK Biobank.
World Health Organization (2023) World health statistics 2023: Monitoring health for the SDGs. Geneva: World Health Organization.
World Health Organization (2023) Global cancer observatory: Cancer today. Lyon: International Agency for Research on Cancer.










